Data-driven decisions strengthening AMR strategy in East and South Africa
Data is a powerful tool in the global effort to tackle antimicrobial resistance (AMR). It transforms disease surveillance into actionable insights and provides the evidence for effective policy decisions. Numbers alone, however, are not enough. For data to truly drive change and offer a clear picture of AMR from local to global levels, it must be standardised, coordinated and reliable.
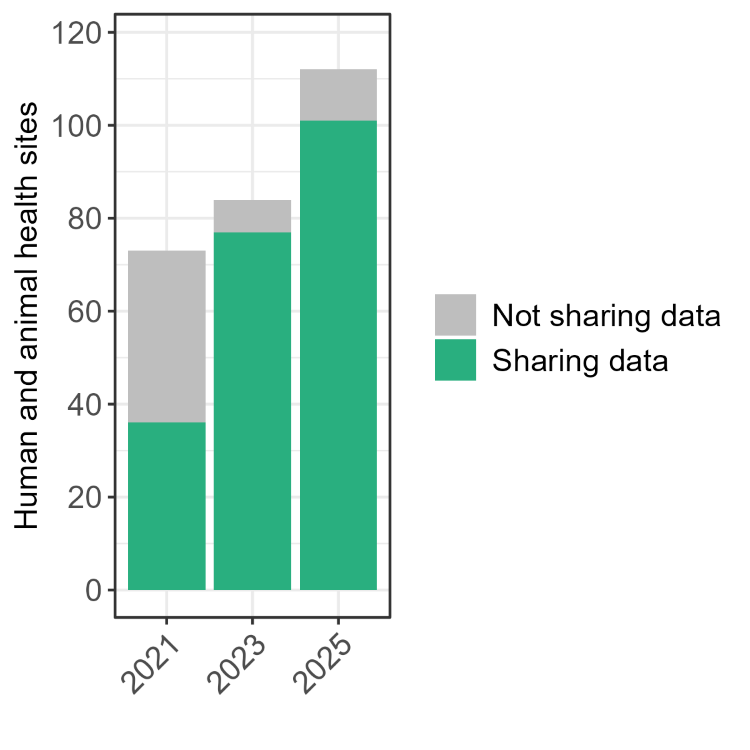
Across East and Southern Africa, Fleming Fund-supported countries have made significant strides in the quality and quantity of AMR data produced, as well as in integrating data with established surveillance systems. These efforts are making AMR data more robust for national action and sharing with international partners.

Above: UK's Department of Health and Social Care's visit to the Ministry of Health in Malawi (credit: Mott MacDonald).
Fragmented to coordinated systems
When the Fleming Fund began its work in 2016, AMR data in many countries were fragmented. Throughout the East and Southern Africa region, the Fleming Fund partnered with Uganda, Tanzania, Kenya, Malawi, Eswatini, Zimbabwe, Zambia, and from 2024, Rwanda. Within the human health sectors of these countries, research institutions and hospitals generated some data, but lacked coordination at the national level.
In the animal health sector, data mainly came from training laboratories and research projects. This data, however, was mostly available in capital cities and not readily accessible to animal health professionals working in rural areas. In both human and animal health sectors, the data shared with international platforms was typically exclusive to resistance patterns – leaving a limited picture of the antimicrobials used, promoted and monitored as underlying factors affecting AMR.
The data landscape has subsequently changed across these countries, with Fleming Fund-supported activities increasing the volume, quality and diversity of AMR data being produced. This provides Technical Working Groups and health officials with evidence to inform policy recommendations, alongside guidance on antimicrobial use (AMU) and antimicrobial stewardship (AMS).
Contributing data to GLASS [...] ensures global AMR strategies accurately reflect resistance patterns in low and middle-income countries ─ where the burden of infectious diseases is often highest.
Ade Olarewaju, Senior Programme Officer for Global Public Health, ASM.
Transforming data into action
As a result of these efforts, Fleming Fund-supported countries in the region have also increased the amount of data uploaded to the World Health Organization (WHO)’s Global Antimicrobial Resistance and Use Surveillance System (GLASS). This demonstrates a commitment to building or strengthening national AMR surveillance systems by generating quality AMR data analysis and sharing locally and globally.
Tanzania, for example, began Fleming Fund activities in 2017 and enrolled with GLASS in 2019, and has consistently submitted data to the platform since. In 2025, Tanzania submitted data to GLASS from 13 sites, including private hospitals, supported by the American Society for Microbiology (ASM), the Fleming Fund Country Grant lead.
Ade Olarewaju, the Senior Programme Officer for Global Public Health at ASM, has observed that preparing data for GLASS has had wide-ranging benefits, with the process requiring systematic, standardised data collection and national-level review.
“This has led to the establishment of standardised data quality assurance mechanisms at both national and facility levels, institutionalised routine data validation and feedback loops with surveillance sites, explained Ade.
“These protocols have strengthened laboratory capacity, improved quality management systems, and increased the overall reliability of AMR data. Contributing data to GLASS, from countries like Tanzania, ensures global AMR strategies accurately reflect resistance patterns in low and middle-income countries ─ where the burden of infectious diseases is often highest.”
WOAH-ANUIMUSE
The region has also consistently collected and reported antimicrobial consumption (AMC) data annually to the World Organisation for Animal Health (WOAH) through the ANIMUSE platform.
The AMC data has been used to inform antimicrobial resistance practice, for example:
- Tanzania, to develop the National Veterinary Standard Treatment Guidelines and the National Action Plan on AMR (2023-2028).
- In Kenya and Malawi, to develop Essential Veterinary Medicines lists.
- In Uganda, to develop the National Veterinary Standard Treatment Guidelines.
- In Zambia, to develop an AMS curriculum for veterinarians and para-veterinarians at the University of Zambia, School of Veterinary Medicine.
- Regionwide, presented at conferences as part of World Antimicrobial Awareness Week (WAAW) ─ educating key stakeholders on patterns of overuse, underuse, and misuse of antimicrobials, such as antibiotic use for produce growth promotion.

During WAAW 2025, the Vice President of the United Republic of Tanzania presented ASM (to Ade Olarewaju, far right) with an outstanding performance and leadership award in recognition of the Fleming Fund grants advancing the country's AMR surveillance efforts (credit: ASM).
Driving policy, practice and reform
AMR data analysis in Zimbabwe found high levels of resistance among Escherichia coli and Salmonella pathogens in broiler chicken samples. The data showing these resistance patterns led to the decision to actively discourage the use of sulphonamides and tetracyclines ─ two common antibiotics used in veterinary medicine and agriculture ─ and to promote more rational antibiotic use among poultry farmers.
The AMC data submitted to the WOAH AMNIUSE platform from Zimbabwe also led to the development of a policy brief on Antimicrobial Stewardship in Zimbabwean Animal Agriculture.
Similarly, in Malawi, surveillance data on resistance to carbapenem, antibiotics used to treat severe bacterial infections, revealed resistance patterns and inappropriate prescribing. The findings were shared with hospital AMS committees and Ministry of Health Technical Working Groups.
Dr Titha Dzowela, Coordinator for the Fleming Fund Country Grant at the University of North Carolina at Chapel Hill (UNC), says that this evidence prompted several actions introduced pre-authorisation and review systems for carbapenem use, updating treatment guidelines, and promoting bacterial culture and sensitivity testing before escalation.
“By linking laboratory surveillance more directly to prescribing decisions, clinicians were encouraged to reserve carbapenem antimicrobials for confirmed or strongly suspected multidrug-resistant infections. This contributed to a 14% reduction in carbapenem use between 2021 and 2025,” said Dr Titha.
In Kenya, increased AMR data has catalysed institutional and policy reform, with the country’s National Public Health Institute established as a hub for AMR-related activities. Deborah Nanjebe, the Fleming Fund microbiologist and laboratory specialist for the East and Southern Africa region, said: “I have seen health policymakers in Kenya elevate AMR to the same risk category as global security threats; this move will strengthen resource mobilisation for AMR in the future.”
Central database for human and animal health data, shared from Fleming Fund-supported countries in East and Southern Africa (credit: Mott MacDonald).
Sustaining AMR progress
Countries across the East and Southern Africa region have made remarkable progress in improving the quality and quantity of AMR data. Yet sustainability remains a challenge. Surveillance systems rely heavily on skilled personnel for sample collection, analysis, and data sharing, and with limited AMR funding streams, governments struggle to secure long-term financing.
AMR is not an isolated issue and is deeply interconnected with broader health systems. Investments in AMR data infrastructure strengthen surveillance and enhance the capacity to respond swiftly to infectious diseases and health security threats. Deborah added: “As the experience of Fleming Fund-supported countries shows, quality data is not just information; it is the foundation for informed and meaningful action.”
GLASS tool WHONET
A Fleming Fund Regional Grant also supports the international WHONET project, a free WHO platform that helps laboratories manage and analyse AMR data. WHONET enables data to flow from individual sites into national repositories, supporting the production of national antibiograms; critical summaries of AMR patterns that guide treatment protocols and inform health policy decisions.
“The Fleming Fund-supported countries in the East and Southern Africa region successfully collect WHONET data from microbiology laboratories to support local, national, and regional perspectives, said Dr John Stelling, Co-Director of WHONET. “This enables weekly automated data processing and reporting, which has strengthened early detection systems by providing timely alerts on priority public health findings requiring investigation or response.”

Sharing antibiogram at a clinical meeting with the surgical team at Zomba Central Hospital in Malawi (credit: UNC).
More Like This
In a significant milestone for antimicrobial resistance (AMR) surveillance in Pakistan, the Fleming Fund Country Grant (FFCG), led by DAI, in collaboration with the Ministry of National Food Security & Research (MoNFS&R), has developed the country’s first ‘National Surveillance Strategy for AMR in Aquaculture’.
Since 2019, Fleming Fund grantee, International Vaccine Institute (IVI), has led the CAPTURA consortium to expand the volume of historical data for antimicrobial resistance (AMR), consumption (AMC), and use (AMU) across 12 countries in South and Southeast Asia.